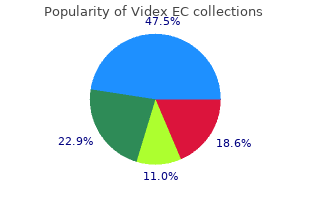
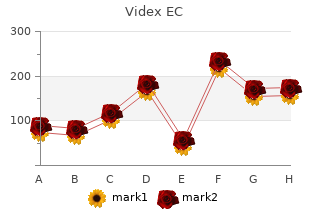
Videx EC
", medicine administration."
By: James Andrew Alspaugh, MD
- Professor of Medicine
- Professor in Molecular Genetics and Microbiology
https://medicine.duke.edu/faculty/james-andrew-alspaugh-md
Intra-operative enteroscopy probably the most invasive but probably the most delicate method of small bowel imaging is intraoperative enteroscopy , which is performed during open laparotomy or, much less commonly, via laparoscopy (Yamamoto et al 2001). This approach requires the patient to be underneath common anaesthesia as the surgeon inserts the enteroscope both transanally and/or transorally or by way of an operative enterotomy, relying on the world of interest and physician choice. Through an abdominal incision, the surgeon then guides the gut over the endoscope (Carey & Fleischer 2005). Is double-balloon enteroscopy as safe as, or safer than, laparotomy with or without intra-operative enteroscopy at figuring out and treating obscure gastrointestinal bleeding or suspected small bowel illness? Is double-balloon enteroscopy as, or extra, effective at figuring out and treating obscure gastrointestinal bleeding or suspected small bowel illness in comparison with laparotomy with or without intra-operative enteroscopy? Is double-balloon enteroscopy as, or extra, price-effective at figuring out and treating obscure gastrointestinal bleeding or suspected small bowel illness in comparison with laparotomy with or without intra-operative enteroscopy? Appendix C describes the electronic databases that have been used for this search and the other sources of evidence that have been investigated. Inclusion/Exclusion standards the standards for including articles on this report various relying on the type of research query being addressed. Often a research was assessed greater than as soon as as a result of it addressed a couple of research query. If there was any doubt concerning inclusion of papers, this was Double-balloon enteroscopy 9 resolved by group consensus to make sure that all potentially related studies have been captured. The inclusion standards related to each of the research questions posed on this assessment are supplied in Boxes 1 and a couple of in the outcomes section of this report. Figure four Study choice course of Phase 1 All reference citations from all literature sources have been collated into an Endnote eight. Phase four Inclusion standards have been independently utilized to the total-textual content articles by one Phase 5 the reference lists of the researcher. Those articles included articles have been pearled assembly the standards shaped part for extra related studies. The these have been retrieved and the rest supplied background assessed based on part four. Phase 6 the evidence base consisted of articles from phases four and 5 that met the inclusion standards. These dimensions (Table 2) consider essential aspects of the evidence supporting a particular intervention and embody three major domains: strength of the evidence, measurement of the effect and relevance of the evidence. The first domain is derived immediately from the literature identified as informing a particular intervention. Table 2 Evidence dimensions Type of evidence Definition Strength of the evidence Level the research design used, as an indicator of the diploma to which bias has been eradicated by design. Statistical precision the p-worth or, alternatively, the precision of the estimate of the effect. Size of effect the gap of the research estimate from the ?null worth and the inclusion of only clinically essential effects in the confidence interval. Relevance of evidence the usefulness of the evidence in medical follow, notably the appropriateness of the result measures used.
Syndromes
- Gently rocking the child
- Abscesses
- General joint aches
- Bleeding underneath the scalp (cephalohematoma) caused by a difficult delivery
- Complete blood count (CBC)
- Ischemic cardiomyopathy
- Is there bloody urine or blood in the stools?
- Severe pain or burning in the nose, eyes, ears, lips, or tongue
- Nerve conduction velocity test
Annals of Transcatheter valve-in-valve aortic valve Thoracic Surgery 2008;86(1):forty six-fifty four; implantation: sixteen-month follow-up . Feasibility and preliminary Percutaneous valve-in-valve procedure for results of percutaneous aortic valve extreme paravalvular regurgitation in aortic implantation including number of the bioprosthesis. American Journal of Cardiology Results of transfemoral or transapical aortic 2008;102(9):1240-1246. Journal Severe valvular regurgitation and late of the American College of Cardiology prosthesis embolization after percutaneous 2009;fifty three(20):1855-1858. Percutaneous transcatheter aortic valve replacement: first transfemoral implant in Asia. Transfemoral aortic valve implantation Surgical aspects of endovascular retrograde with pre-existent mechanical mitral implantation of the aortic CoreValve prosthesis. Cardiovascular Interventions Combined transapical aortic valve 2007;70(4):610-616. Catheterization & Transapical transcatheter mitral valve-inCardiovascular Interventions 2007;sixty nine(1):56valve implantation in a human. Implantation of the CoreValve percutaneous First report on a human percutaneous aortic valve. Annals of Thoracic Surgery transluminal implantation of a self2007;eighty three(1):284-287. Catheterization & Cardiovascular profitable transapical aortic valve Interventions 2005;sixty six(4):465-469. Percutaneous implantation of the CoreValve self-expanding valve prosthesis in high-danger 86. Wenaweser P, Buellesfeld L, Gerckens U, patients with aortic valve disease: the et al. Catheterization & Percutaneous aortic valve replacement for Cardiovascular Interventions extreme aortic stenosis in high-danger patients 2007;70(5):760-764. Successful percutaneous coronary intervention after implantation of a CoreValve percutaneous aortic valve. Implantation of two self-expanding aortic First human case of retrograde transcatheter bioprosthetic valves throughout the same implantation of an aortic valve prosthesis. Delayed improvement in valve Catheterization & Cardiovascular hemodynamic efficiency after Interventions 2009;73(2):161-166. Annals of Thoracic Surgery Procedural success and 30-day clinical 2008;85(5):1787-1788. Circulation: Cardiovascular Treatment of extreme regurgitation of Interventions 2008;1:126-133. Successful percutaneous administration of left Catheterization & Cardiovascular primary trunk occlusion throughout percutaneous Interventions 2009;73(5):713-716. Percutaneous aortic valve replacement in Transcatheter Cardiovascular Therapeutics two cases at high surgical danger: procedural Conference, 2008.
Host Susceptibility Factors Not all parasitic an infection causes disease of scientific significance . Metabolic means of the parasite, particularly the character of any waste products or toxins produced by the parasite during its development and copy. Escape mechanism of parasite from the immune system That parasitism is extensive unfold in nearly all species of animals would indicate that parasites have developed the capacity to escape or render ineffective the host internal defense mechanisms. Thus Schistosome worms are capable of masking their foreigners by buying a surface layer of host antigens which probably protect them from antibody injury. This phenomenon of antigen sharing between a parasite and a number known as Molecular mimicry. This generally, leads to an increase in the severity of any viral or bacterial an infection additionally current. Immuno-supression is due to production by the parasite of enormous portions of soluble antigens which: 3. Induce B or T-cell tolerance both by blocking antibody forming cells or by depleting the inventory of mature antigenspecific lymphocites ( clonal exhaustion ). Indirect Life Cycle: When a parasite requires an intermediate host or vector to complete its growth. To overcome this problem, a binomial scientific title is used, consisting of a generic and a selected designation primarily based on the International Code of Zoological Nomenclature. The first title in the binomial is that of the genus to which the organism belongs, and the second is that of the species. This combination of in designating an animal or plant species is termed binomial nomenclature. Taxonomic classification of medically essential parasites of man belong to the dominion of Animalia and most parasites are members of three phyla: Phylum Protozoa Phylum Platyhelminths and Phylum Nemathelminths. Parasitology 24 Basic Classification of Parasites of Medical Importance Kingdom Animalia I I I I Sub-kingdom Protozoa Metazoa I I I I I I I Phylum Protozoa Platyhelminthes I Arthropoda I I Nemathelminthes I Class I 1) Trematoda I I I 2)Cestoda I 1) Insecta, 1) Rhizopoda 2) Arachnid, 2) Zoomastigophora I etc. Discuss the characteristics of each class of protozoan parasite generally and every parasite specifically. Apply the necessary procedures for the analysis of protozoan parasites and be capable of determine them in the procedures used. Introduction Protozoa consists of an unlimited assemblage of single cell micro-organisms that are positioned in the subkingdom, or phylum protozoa. They are made of a mass of protoplasm differentiated in to cytoplasm and nucleoplasm. The ectoplasm function in safety, locomotion, ingestion of meals, excretion, respiration. The protozoa of medical importance to humans embody Amoebas, Flagellates, Ciliates, Coccidia, sporozoa and Microsporidia. For this reason the laboratory technician must be conversant in attribute of pathogenic as Parasitology 27 well as non-pathogenic species. Protozoa could colonize or infect intestinal tract, pharynx, and the uro-genital tract of humans.
Maintaining Volume Status/Hydrasupport , their large dimension and limited durability hindered tion. There have been quite a few stories of comfort and enhanced quality of life, and a reduced an infection extended help with these units and with promising 1,7,eight,12?16 risk. Thus, patient selection ties that vary in severity, depending on the extent and and the timing of implant are two of the most important period of heart failure. The present 6-month survival information for patients erations within the patient-selection course of. Within hours 2 ?Progressive decline?inotrope dependence with persevering with deterioration. Within a number of days three ?Stable however inotrope dependent?describes scientific stability on mild-to-moderate doses Within a number of weeks of intravenous inotropes (patients steady on short-term circulatory help with out inotropes are within this professional? The survival to hospital discharge instability, major coagulopathy, prolonged need for mewas 87. Examples of factors that may preclude implant embody a ?excessive-risk how a patient?s risk rating is determined are provided in classi? Overall risk components for operative mortality tients who initially present as excessive-risk or very excessive-risk are A number of investigators have developed operative mormost prone to bene? Thus, composite risk scores can be used to implant before their situation worsens. Pre-operative risk components associated with the highVasodilator therapy 4 est risk of death had been extreme functional impairment, markers Mean pulmonary artery pressures 25 mm Hg three of worldwide cardiac dysfunction, finish-organ injury, and malAspartate aminotransferase forty five U/ml 2 nutrition. Obesity paradox severe adverse occasions similar to bleeding, renal failure, and Obesity is common in patients with heart failure. Two recent research have reported predictive models Parameters to contemplate for evaluating right-heart func35,36 tion are listed in Table 6. In 1 examine, inotropic help 14 days post-operatively was required in 38% of advance nutrition help while addressing the metabolic 2 imbalances associated with heart failure. Malnutrition is quite common in patients calculated using this method: with superior heart failure. Other non-routine tests that may be performed are rectal swab for vancomycin-resistant enterovirus, nasal swab for Staphylococcus an infection, peripheral blood cultures, and plasma levels of free hemoglobin. A detailed pre-operative nutrition assessment kind 15 mg/dl, enteral feedings are sometimes helpful pre-operacan be found in Appendix A. Several recent stories have additionally 29 supported patients have been previously published. Markshown that patients with a pre-albumin 15 mg/dl at 2 weeks after implant are at excessive risk of dying before dis30 cost. Table eight Minimal Pre-implantation Goals Diets must be liberal and embody oral dietary supplements, Parameter Desired worth meals from home, and between-meal snacks. When possible, patients should take multivitamins, iron dietary supplements, and Renal Blood urea nitrogen forty mg/dl erythropoietin.
. Erectile Dysfunction- Learn A Natural Method For Long-Lasting Erections No DRUGS.